

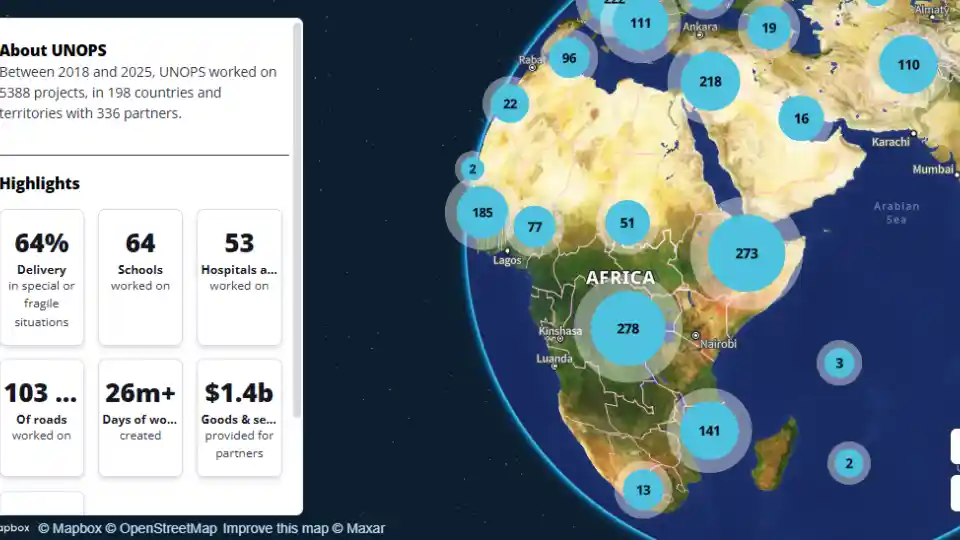








The United Nations Office for Project Services (UNOPS)

Stamping out malaria for good
Health workers and scientists are up against the clock to put an end to malaria in the Greater Mekong Subregion (GMS) once and for all. For many years, the region has been the epicentre of antimalarial drug resistance – a phenomenon that is threatening to thwart malaria control efforts globally.
Transmitted by the bite of an infected mosquito, malaria is one of the deadliest diseases in human history.
The most dangerous form of malaria is caused by the Plasmodium falciparum parasite. It is also the most common. Left untreated, it can be fatal. More concerning yet, in parts of the GMS region, this particular parasite has developed resistance to many artemisinin-based combined therapies (ACTs) – the most effective treatments in use today.
Photos
- ©UNOPS/Elise Laker

Some 216 million cases were recorded in 2017 and it is estimated to have been responsible for 435,000 deaths, with 93 per cent of those occurring in Africa, where the disease is still a major killer of children under five.
Efforts are being intensified throughout the region to eliminate the disease and prevent these resistant strains from spreading to other regions like Africa, which bears the brunt of the world’s malaria burden.
Multi-drug resistant malaria first emerged in Pailin, Cambodia near the border with Thailand in 2008, and soon spread to China, Laos, Myanmar, Thailand and Vietnam. However, resistance to single-drug treatments has previously occurred in this area. In the 1950s, Chloroquine, a highly effective antimalarial at the time, started becoming less efficient and by the 1980s, resistant strains had spread to Africa, making an already dire situation worse. Since then, resistance to new malaria treatments seems to keep on occurring in the Cambodian border town.
The World Health Organization currently recommends five ACTs to treat Plasmodium falciparum malaria, but in Cambodia, the parasite has already developed resistance against four out five of these medicines. While the exact reason why Cambodia is the unlikely source of resistance continues to baffle scientists, the gravity of the situation is fully understood.
For public health specialists like Naeem Durrani, a programme coordinator for UNOPS specializing in malariology, there is a huge sense of urgency to eliminate malaria in the area.
“This region is at risk of losing all of the drugs that are effective against malaria. If that happens, we have a real public health emergency on our hands,” says Naeem.
What is artemisinin?
- Artemisinin was discovered in 1972 and has been hailed as a magic drug by many due to its effectiveness in treating malaria. It is derived from the Artemisia annua or sweet wormwood plant, which has traditionally been used in Chinese herbal medicine. Artemisinin continues to serve as the foundation for malaria treatment, with artemisinin-based combined therapies currently the medicine of choice to treat uncomplicated malaria.
According to Naeem, as long as these multi-drug resistant strains exist, there is always the potential for them to spread beyond the region’s borders to places where health infrastructure is even less equipped to deal with such an outbreak.
“It would be a catastrophe if these strains reach Africa for example. Many lives will be claimed, especially children. We cannot mess around – the answer is to eliminate,” says Naeem.
Naeem oversees the funds for the second phase of the Regional Artemisinin-resistance Initiative (RAI) – RAI2 Elimination – in Cambodia. The three-year programme, which is funded by the Global Fund to Fight AIDS, Tuberculosis and Malaria, was set up in 2017 to accelerate efforts to eliminate Plasmodium falciparum malaria in the GMS. Prior to this, there had been significant progress in malaria case reduction, with the number of reported cases falling by 75% since 2012. Many remote areas, however, remain highly endemic.
“In elimination settings, as malaria decreases, the remaining cases are always found in extremely hard-to-reach places. They will be somewhere in the far flung areas of the mountains, across rivers, in the forests,” says Naeem.





The humid conditions of the forest provide the perfect conditions for mosquitoes to thrive – roughly half of the world’s population at risk from malaria lives in forested areas. In recent years, Cambodia’s northeast, with its sparse population and dense, resource-rich forests, has been attracting more and more migrants in search of economic opportunities. Logging, land clearing, construction and the collection of various forest products, such as mushrooms and bamboo, are common.
Use of the forest is constantly changing depending on accessibility, climate and market demand for particular products. In 2017, for example, the appearance of the samrong, a rare fruit that grows every four to five years, resulted in people rushing deep into the forests. And while they may have been rewarded financially for their efforts, they paid a high price in terms of health, as many caught malaria.
As part of heightened efforts to curb malaria among the migrant populations, a mobile migrant population tracking system is in place to help identify and predict the movement of people so that pop up testing stations, outreach and other activities can be dispatched quickly.
“We have to follow closely the pattern of movement of people. It all depends on the season and what types of products are available in the forest,” explains Yves Bourny, the director of the Cambodia office of the Malaria Consortium, one of several implementing partners.

The malaria post at an unofficial border crossing in Okouk village, Stung Treng Province is one such example. The crossing, which borders Laos, is run by local health volunteers Ken Sreyleak and Choy Dom. Sreyleak has worked as a volunteer for nine years, accessing hard to reach communities on her motorbike. Over the years, she has seen the number of malaria cases go down in the area.
“Before, 70 people on average used to test positive for malaria every month. Now, it’s about 30. My work can be challenging though as the road conditions are not good,” says Sreyleak.


Many of the people coming to be tested work on a nearby construction site. Seang Hean moved to Okouk from the capital, Phnom Penh, for work and heard about the malaria post from a friend. It is his first time being tested for the disease and this time the results are negative. The ever increasing flow of migrants moving to the area in search of work means that response teams need to act quickly to prevent malaria from spreading.
Population movement is a major contributing factor in malaria transmission. A person who goes untreated with malaria can transmit the infection to malaria-free mosquitoes if they are bitten again. This can lead to an outbreak of malaria. A team of locally trained community health volunteers like Sreyleak and Dom provide on the spot testing, diagnosis and treatment for migrants and forest goers working in hard-to-reach malaria hotspots so that they can receive treatment quickly before the disease has time to spread. The volunteers also provide preventive care such as insecticide-treated bednets and health education as well as referrals when cases are severe.






Across the border in Laos, the story is similar. The situation, according to Dr. Bouasy Hongvanhthong, the director of the Center for Malariology, Parasitology and Entomology (CMPE), has greatly improved.
“In the last few quarters, no malaria cases have been reported in 80 out 145 districts. This is evidence that we’re continuing to make good progress,” says Dr. Bouasy Hongvanhthong.
The country, along with its neighbours Cambodia and Vietnam, has pledged to eliminate the deadly Plasmodium falciparum malaria parasite by 2025 and all species of malaria by 2030, and it seems to be on track. Since 2010, the number of malaria cases in Laos has declined by 61 per cent. Like in Cambodia, there is a strong focus on the hard-to-reach populations in the mountainous regions and the remote forested areas along the Mekong river. In 2018, to ensure malaria trends continue to go in the right direction, the CMPE trained more than 2,000 health workers and 1,500 village malaria workers in malaria control and elimination.
“We need to make sure people continue to report correctly even when malaria cases are going down. People tend to pay less attention when the number of cases decreases,” says Dr. Bouasy.
“The number of soldiers affected by malaria has decreased a lot compared to the past. Our medical staff are trained and have the right equipment and medical supplies to deal with cases as and when they arise.”

Eliminating malaria means reaching all people, no matter how hard to access. One of the programmes currently being implemented by the CMPE is targeting the military. They are considered a high-risk group because their work often requires them to spend large amounts of time deep in the forest. Reporting information about the military is sensitive, which means mapping malaria cases can be difficult, but training and the provision of medical supplies as well as preventative measures like bednets and mosquito repellent are helping to reduce cases among military personnel.
The road ahead in eliminating malaria in the GMS countries is no doubt a challenging one, but with malaria cases continuing to go down those working towards its elimination remain positive that it can be wiped out in the not so distant future.




Project details
The Regional Artemisinin-resistance Initiative 2 Elimination (RAI2E) programme is a $243 million regional grant to accelerate the elimination of Plasmodium falciparum malaria in the Greater Mekong Subregion between 2018 and 2020. RAI2E supports increased malaria service coverage for remote populations in border areas and other at-risk populations, as well as case management through health volunteers and strengthening of national surveillance systems.
UNOPS is responsible for managing the funds of the project and providing quality assurance as well as monitoring and evaluation. The programme is being implemented by 34 partners across the region and is funded by the Global Fund to Fight AIDS, Tuberculosis and Malaria.
The programme in Cambodia is implemented by CARE, Catholic Relief Services, Health Poverty Action, the National Center for Parasitology, Entomology and Malaria Control, Malaria Consortium, Partners for Development and Population Services International.
In Laos, UNOPS has been working in partnership with the Ministry of Health, the World Health Organization and civil society organizations to support the country’s malaria control and elimination efforts.
Access to locations in Laos highlighted in this article has been made possible through the support of the government of Laos, Lao Positive Health Association and the Ministry of Health (Department of Planning and International Cooperation, Department of Communicable Disease Control, and Centre for Malariology, Parasitology and Entomology).





